
This version of the Canadian Accessibility and Remoteness Index (CARI+) measures access to public high schools in Canada via travel time and distance.
Rural obstetrical care in Canada has limited local access, meaning many women must travel, sometimes over several hours, to give birth. Care is often provided by fewer specialists and more family physicians, and services vary widely between communities. These gaps can affect outcomes and reflect that rurality is a key social determinant of health.
There are fewer obstetrical specialists in rural areas, so care depends heavily on family physicians and limited staff, which affects consistency of care. Birth services are provided by a wide range of individuals, which differs by province. Midwives, labor and delivery doctors or nurses, doulas and OBGYN’s all provide birth care to labouring mothers.
Limited access to the appropriate level of care can lead to worse birth outcomes, increased stress, and financial strain due to travel. It also impacts overall health because rurality acts as a social determinant of health, affecting both mothers and newborns. Long travel times can lead to delayed care, emergency deliveries, and higher stress, which can affect outcomes. Rural access issues are often more severe for remote Indigenous populations, where women may have to leave their communities weeks before birth, impacting cultural safety and family support.
Recognition matters because rural care is an underrepresented but widespread issue in Canada. Acknowledging it helps drive policy changes, resource allocation, and improved access to care, which can lead to better maternal and newborn outcomes.
Calculation of the CARI+
This CARI+ index measure was calculated using the general methodology for CARI+, as described in Canadian Geographies / Géographies canadiennes. This methodology was adapted to calculate accessibility to hospitals offering obstetrical services and birth centres across Canada. It was achieved by measuring from population-weighted Dissemination Area (DA) centroids to birth centres as service centre locations.
Lists of hospitals and publicly-funded birth centres and the level of care were obtained and validated from provincial ministry of health websites. Inclusion criteria consisted of regional and community hospitals that had an obstetrical ward, or other birth centres. Other birth centres include midwifery-led free-standing clinics separate from hospitals, Indigenous midwifery-led birth centres, or hospital-attached alternative birth centres. The options available for expectant mothers differ by Province.
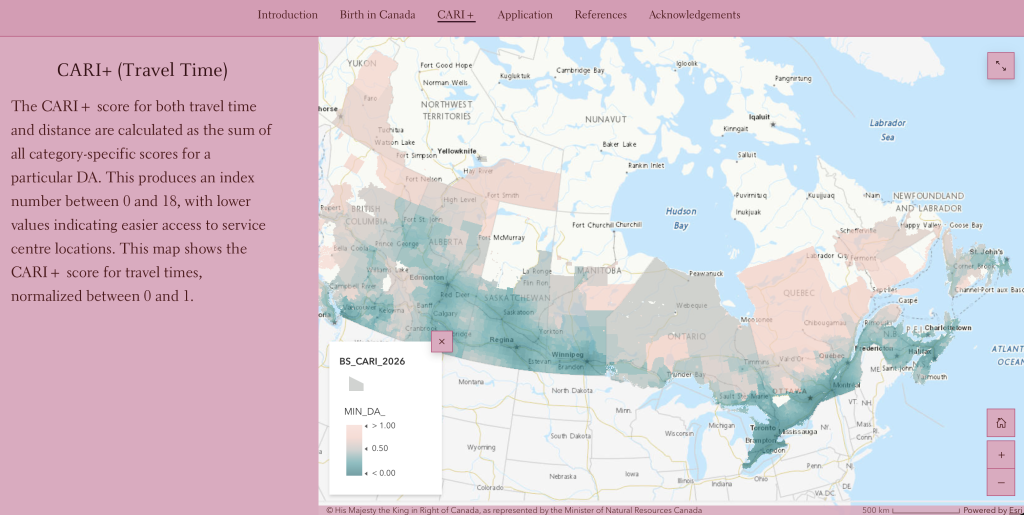
The CARI+ score for both travel time and distance are calculated as the sum of all category-specific scores for a particular DA. This produces an index number between 0 and 18, with lower values indicating easier access to service centre locations. This map shows the CARI+ score for travel times, normalized between 0 and 1.
Interpretation
Limited rural birth services place increased pressure on regional centres, as many women must travel to urban hospitals for delivery. This leads to higher patient volumes, resource strain, and greater demand on staff and facilities. Regional centres must also manage more high-risk and transferred patients, which can impact wait times and quality of care. The shift from local to centralized services creates capacity challenges and system strain in larger hospitals while rural communities lose access to care.
Urban populations may also be affected as increased demand from rural patients can lead to overcrowding, longer wait times, and stretched healthcare resources in city hospitals. This added pressure may impact the quality and timeliness of care for urban residents as well. While urban areas have more specialized services, the increase of rural patients contributes to system strain and resource competition.
The results reinforce that rural obstetrical care is a system-wide problem influencing equity and accessibility to care by allowing people to observe how underserved rural populations affect regional and urban centers. By mapping rural and urban differences, this StoryMap highlights where service gaps, long travel distances, and provider shortages exist. This can help inform healthcare planning and policy decisions, such as where to invest in rural maternity services, improve transportation systems, or expand provider availability.
Definitions and Limitations
Birth Services: Options for birth in Canada include hospitals (maternal and newborn care), free-standing birth centres (usually staffed by midwives), alongside midwifery units (attached to hospitals), or midwifery-support home births. However, availability of these services varies greatly depending on the city, region, and province.
Levels of Care (LOC): In Canada, obstetrical services are organized into tiered levels of care (often called levels or tiers of service) that range from basic community care to tertiary specialized centres. This regionalized framework ensures that pregnant women and newborns receive risk-appropriate care as close to their home communities as possible.
- Level I (Low-Risk / Basic Care): Provides care for healthy, low-risk pregnancies with an anticipated uncomplicated birth (36 weeks gestation or later). These community or rural hospitals are staffed by midwives, family physicians, or general practitioners, and typically offer routine labor, delivery, and postpartum care.
- Level II (Moderate-Risk / Specialty Care): Handles low- to moderate-risk pregnancies, including conditions like gestational hypertension, mild pre-eclampsia, or uncomplicated multiple pregnancies (e.g., twins). These centers typically provide on-site access to general obstetricians, pediatricians, and anesthesia, as well as an established Level II Neonatal Intensive Care Unit.
- Level III & IV (High-Risk / Subspecialty Care): Often referred to as tertiary or regional perinatal centers, these hospitals manage the most complex, high-risk pregnancies. They provide 24/7 on-site subspecialists, including Maternal-Fetal Medicine (MFM) specialists, neonatologists, and access to advanced surgical and diagnostic tools. These centers house Level III NICUs capable of caring for critically ill newborns and extremely premature infants (often those born well before 32 weeks).
Selected References
- Canadian Institute for Health Information. Hospital Births in Canada: A Focus on
Women Living in Rural and Remote Areas. Ottawa, ON: CIHI; 2013. - Guliani H. Mix of maternity care providers in Canada. Healthcare policy. 2015 Aug;11(1):46. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4748365/
- McGaughey T, Peters PA. Introducing the Canadian Accessibility and Remoteness Index (CARI+). Can Geogr Le Géographe Can 2026;70. https://doi.org/10.1111/cag.70082.
- Miller KJ, Couchie C, Ehman W, et. al. Rural maternity care. Journal of Obstetrics and Gynaecology Canada. 2012 Oct 1;34(10):984-91. https://doi.org/10.1016/S1701-2163(16)35414-7.